Hypertensive Retinopathy
Hypertension may lead to multiple adverse effects on the eye. Hypertension can cause retinopathy, optic neuropathy, and choroidopathy.
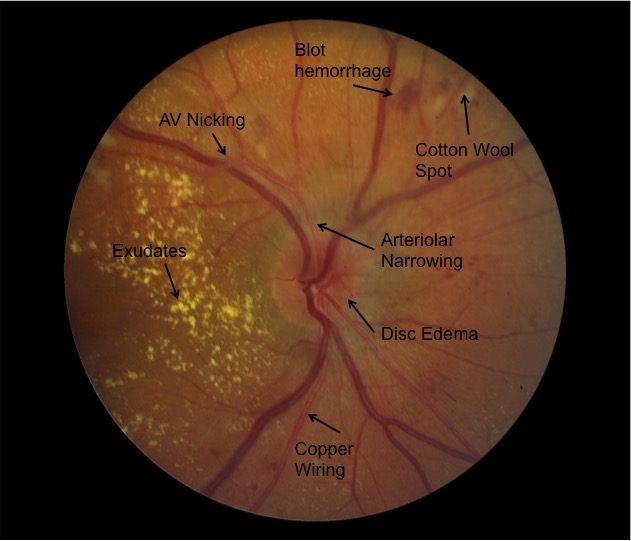
Hypertensive retinopathy is the result of changes to the retinal vasculature in high blood pressure states. Initially, arteriole tone is increased due to autoregulation in the body’s attempt to reduce blood flow, causing the arterioles to narrow. Over time, involved vessels can become sclerotic, with thickened intima and media layers. Eventually, the blood-retina barrier can be disrupted, resulting in exudates and retinal ischemia or hemorrhage. Hypertensive retinopathy includes two disease processes. The acute effect of systemic arterial hypertensive area results of vasospasm to autoregulate perfusion. The chronic effects of hypertension are caused by arteriosclerosis and predispose patients to visual loss from vascular occlusion or macroaneurysms.
RISK FACTORS
- High salt diet.
- Tobacco use.
- Family history.
- Ethnic background.
- Duration of elevated blood pressure.
- The amount of blood pressure elevation over normal.
SIGNS AND SYMPTOMS
- Eye pains.
- Reduced visual acuity.
- Constricted and tortuous arterioles.
- Retinal hemorrhage.
- Hard exudates.
- Cotton wool spots.
- Retinal edema.
- Widening of the arteriole reflex.
- Arteriovenous crossing.
- Copper or silver wire arterioles.
MANAGEMENT
The treatment for hypertensive retinopathy is primarily focused on reducing blood pressure. It is important to work together with the patient’s primary care doctor to ensure timely evaluation and management to reduce ocular and systemic damage. The treatment for moderate to severe hypertensive retinopathy is to reduce the mean arterial pressure by 10-15% in the first hour. Of note, blood pressure should be lowered in a controlled manner and by no more than 25% compared to baseline by the end of the first day of treatment to prevent further ischemic damages to target end organs. Initial treatment often requires parenteral antihypertensive agents and then transitioned to oral agents. Goal systolic blood pressure is <130mmHG and diastolic pressure is <80mmHG over the next 2-3months.